Life Sciences
Stem Cells May Move to the Front Line against Multiple Sclerosis
Researchers maintain that patients with severe multiple sclerosis should be able to receive autologous hematopoietic stem cell transplantation as a first-line…
There is a huge unmet medical need in the treatment of multiple sclerosis (MS), with many neurologists believing that without effective therapies, most patients will never be able to come off disease modifying treatments (DMTs), according to Dame Pamela Shaw, MD, professor of neurology at the University of Sheffield and director of the Sheffield Institute for Translational Neuroscience (SITraN).
Shaw emphasized this point when she spoke at the Third International Symposium on Stem Cell Treatment in Multiple Sclerosis, an event that was held at SITraN on January 20, 2023. Shaw added, “Autologous hematopoietic stem cell transplantation (AHSCT) is transformational for some MS patients, but we need to promote research to show arch skeptics that these types of cell therapy are safe and actually represent good value for money.”
To provide evidence of the safe and effective use of AHSCT to treat MS, Raffaella Greco, MD, senior hematologist in the Blood and Marrow Transplant (BMT) Unit at the IRCCS San Raffaele Hospital in Milan, Italy, and current chair of the European Society for Blood and Marrow Transplantation (EBMT) Autoimmune Diseases Working Party, presented data from the EBMT registry of MS patients treated with AHSCT.

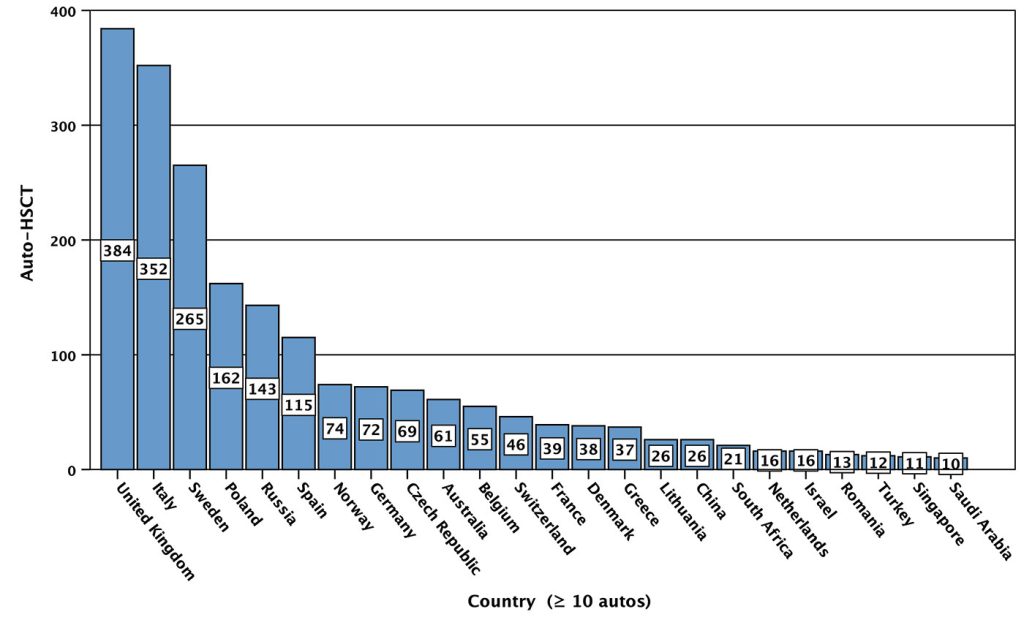
According to Greco, the EBMT registry currently contains data gathered from over 40 countries on more than 4,100 patients that have had AHSCT treatment for autoimmune diseases. “With the 2,100 patients that received AHSCT as a treatment for MS, incidents of death and relapses were low,” Greco stated. John Snowden, MD, director of the BMT Program, Sheffield Teaching Hospitals NHS Foundation Trust, added that the “results from the EBMT registry are helping to build an evidence base for offering AHSCT treatment for MS as a standard everyday practice.”
How and when is AHSCT offered?
With MS, according to the latest set of EBMT guidelines, AHSCT has become an integral and standard-of-care part of treatment algorithms. According to Greco, the EBMT registry shows that England and Italy are the most active countries in Europe for using AHSCT as a therapy to treat relapsing remitting MS (RRMS).
In England, AHSCT is not accessible as a routine therapy because MS treatments are often prescribed following guidelines such as the NHS England Treatment Algorithm for Multiple Sclerosis Disease-Modifying Therapies. This acknowledges AHSCT as a treatment option but recommends it only as a third-line therapy after first- and second-line DMTs fail to control MS symptoms. (These DMTs commonly include interferon β-1a, glatiramer acetate, and monoclonal antibody–based drugs such as alemtuzumab or ocrelizumab.)
Currently, AHSCT in the United Kingdom can be accessed only at specialized centers with expertise in the use of AHSCT. This limits its use to centers in cities such as London and Sheffield. Another reason that AHSCT is offered as a third-line therapy in the United Kingdom is because the efficacy of AHSCT relative to other DMTs has been shown only in one controlled trial (the Multiple Sclerosis International Stem Cell Transplant trial), so many neurologists are not readily informed about its benefits and are skeptical about its safety compared to other approved treatments.
Flipping the pyramid
According to Gavin Giovannoni, PhD, professor of neurology at Barts and the London School of Medicine and Dentistry, a meta-analysis of data from 281 patients that had AHSCT treatment (published by a team led by Imperial College London’s Paolo A. Muraro, MD, PhD) shows that the younger the patient, and the fewer other DMTs they have had, the better their outcomes. Giovannoni also proposed that more frequent measurement of brain volume to predict clinical outcomes of treatments might be useful, noting, “If I had MS, I’d want treatments that normalized my brain volume mass.”
Giovannoni noted that several studies have shown that brain volume loss is linked with increasing clinical disability. This observation, he continued, suggested that stopping excessive brain volume loss could slow disease progression.
“Currently, MS patients are allowed to accumulate a number of disabilities before they can have the most effective treatments, and that is not right,” Giovannoni continued. “We should be treating MS like stroke, where time is of the essence. And we should be offering newly diagnosed patients the most effective treatments such as monoclonal antibody–based therapies and AHSCT first to prevent too much organ damage.”
Giovannoni maintained that flipping the treatment pyramid to provide the most effective treatments first has made huge improvements in treating other autoimmune diseases such as rheumatoid arthritis, and that doing so has also improved outcomes with some cancers. Despite these improvements, the idea of flipping the treatment approach is not accepted with MS.
He also cited poll results indicating that most MS patients expressed a willingness to accept the risks associated with AHSCT. (These results, which appeared on Barts’ blog page, indicated that over 89% of 244 MS patients said that they would like to be offered AHSCT as a first-line therapy.) Sounding an optimistic note, he related, “We have recently changed the protocol of the StarMS trial to allow study subjects to potentially access AHSCT as a first-line therapy.”
The benefits and downsides of AHSCT
“In Sweden, we have been performing open trials of AHSCT with RRMS patients,” said Joachim Burman, PhD, adjunct senior lecturer at the Department of Medical Sciences, Experimental Neurology, Uppsala University. “Over six years, we have seen that more than 60% of patients show no evidence of disease activity (NEDA). NEDA is characterized by no increase in disability, no relapses, and no brain lesions seen with MRI scans.”
Keen to address AHSCT’s safety, Burman cited meta-analyses of AHSCT trials that identified AHSCT’s most common adverse events. There have been cases of immune thrombocytopenia, herpes zoster, and thyroid disease. “The mortality rate from AHSCT is low—around 0.19%,” he emphasized. “[This] is less than the mortality rate from a hip replacement, which is currently 0.3%.”
Burman also discussed the benefits of AHSCT, citing the Multiple Sclerosis International Stem Cell Transplant trial, which was led by Richard Burt, MD, from Northwestern University. This trial of 110 RRMS patients (73 women and 37 men) was the first randomized AHSCT trial, and it compared AHSCT with standard DMTs. Patients with an Expanded Disability Status Scale of 2–5.5 were chosen as study participants. Burman said, “After five-year follow-up, 3 of the 55 patients given AHSCT had disease progression compared to 35 out of the 55 patients that were given DMTs.”
Burman stated that AHSCT has a positive effect on brain health. Specifically, AHSCT slows damage to the brain. “Neurofilament light (NFL) chains are a marker of axonal injury in MS, and due to improvements in analytical methods, we can now measure these in the blood,” he detailed. “In Sweden, my colleagues and I studied 46 patients that were treated with AHSCT, and we found that over two years, the presence of NFLs decreased from 72% to 24%. Over four years, we saw no NFLs in the blood at all, indicating that neuronal damage had been completely halted.”

“DMTs to treat MS are expensive, and patients must take them throughout their lives,” Burman observed. “All the evidence to date indicates that AHSCT is effective for treating RRMS patients.
“Because disease progression can be stopped in many patients, they do not have to take disease-modifying drugs,” he continued. “The cost of AHSCT can become cost-neutral in two to three years.
“We know that up to 14% of MS patients have an increased risk of disability and disease progression, yet in Europe, only around a third of these patients are being given the most effective treatments. Aggressive disease warrants aggressive treatment, and AHSCT offers these patients the best chance of halting their disease.”
The StarMS trial
Despite the body of evidence indicating that AHSCT is safe and effective for many RRMS patients, randomized, controlled trials are needed to generate data to show that it offers better outcomes than less aggressive DMT options.
One such trial is the Autologous Stem Cell Transplantation versus Alemtuzumab, Ocrelizumab, Ofatumumab, or Cladribine in Relapsing Remitting Multiple Sclerosis (StarMS) trial, which is in progress in the United Kingdom. StarMS is funded by the U.K. National Institute for Health and Care Research, and it is led from Sheffield by Basil Sharrack, MD, PhD, consultant neurologist and head of the MS Research Clinic. StarMS is currently aiming to recruit 198 patients aged 16–55 at 19 sites across the United Kingdom. For all participants, there will be a two-year follow-up period. Blood tests, neurology examinations, and questionnaire responses will be evaluated to determine if there is NEDA.
Snowden gave an update on the trial’s progress: “We are aiming to treat around 100 RRMS patients with AHSCT in the StarMS study. We have recruited 18, and we have 25 that have consented. We hope to have 40 people in the trial by April 2023.”
For this trial, patients in the AHSCT arm are being treated with cyclophosphamide and granulocyte colony-stimulating factor (G-CSF) to stimulate stem cell production prior to “harvesting” by apheresis and cryopreservation. Patients then undergo “conditioning” with cyclophosphamide/antithymocyte globulin (ATG), which ablates the bone marrow and immune system, taking out the cells causing autoimmunity issues.
After conditioning has been completed, the stem cells are thawed and infused back into the patient’s bloodstream, rebuilding the bone marrow and reconstituting the defective immune system.
“The reasoning behind using a cyclophosphamide/ATG conditioning regimen rather than BEAM/ATG in the StarMS trial is that cyclophosphamide/ATG has been shown to have a similar efficacy but is less toxic,” Snowden explained. “We hope in the future to have even less toxic regimens to use in AHSCT therapy. In the United Kingdom, we can perform AHSCT for around £35,000 ($43,000) per patient. So, from a health economics point of view, AHSCT to treat RRMS is cost-effective compared to modern DMTs.
“We need as many eligible patients as possible to be put forward for the StarMS study to finish this. Data from this and other trials like it will provide evidence to show that AHSCT is as effective as expensive DMTs, and that AHSCT could be offered as a first- or second-line therapy for many severe RRMS patients rather than as a last resort, which it is in many centers now.”
Sue Pearson, PhD (sue.pearson@internationalsciencewriter.com), has been writing for GEN as a European correspondent since 2001.
The post Stem Cells May Move to the Front Line against Multiple Sclerosis appeared first on GEN – Genetic Engineering and Biotechnology News.












Wittiest stocks:: Avalo Therapeutics Inc (NASDAQ:AVTX 0.00%), Nokia Corp ADR (NYSE:NOK 0.90%)
There are two main reasons why moving averages are useful in forex trading: moving averages help traders define trend recognize changes in trend. Now well…

Spellbinding stocks: LumiraDx Limited (NASDAQ:LMDX 4.62%), Transocean Ltd (NYSE:RIG -2.67%)
There are two main reasons why moving averages are useful in forex trading: moving averages help traders define trend recognize changes in trend. Now well…

Asian Fund for Cancer Research announces Degron Therapeutics as the 2023 BRACE Award Venture Competition Winner
The Asian Fund for Cancer Research (AFCR) is pleased to announce that Degron Therapeutics was selected as the winner of the 2023 BRACE Award Venture Competition….
