Markets
Diabetes Has an Equality Problem: The Healthcare Satisfaction Survey
Our new survey reveals how profoundly race, ethnicity, and income disparities affect the diabetes care that Americans receive.
Race, ethnicity, wealth — these factors play far too large a role in American healthcare. It’s a sad situation that has a big effect within the diabetes community.
Much has been written on the complex causes and consequences of these systemic inequities, but we wanted to learn how people with diabetes really feel about the care they receive today, right now, in the year 2022. To that end, we convened a panel of regular people with diabetes to help assess the nature and scope of healthcare inequality.
Our survey was not powered to evaluate major diabetes outcomes, like A1C or the development of advanced complications. Instead, we homed in on the little things: Does your doctor help you feel better about your condition, or worse? Can you access new medications and technology? Do you have faith that your medical team has the expertise to help you thrive?
Unfortunately, but unsurprisingly, we confirmed that there are sharp racial and socioeconomic lines dividing the diabetes community.
The Healthcare Satisfaction Survey
On Nov. 4, in celebration of Diabetes Awareness Month, we announced the completion of a new survey that aimed to assess how satisfied regular Americans with diabetes are with the medical care and attention they receive. We collaborated on the effort with our friends at Thrivable, a market research platform that engages panels of people with chronic health conditions.
Diabetes is tough, and we know that not everyone gets the support they need. As one of our panelists put it: “They make it seem like it’s an easy thing to do to manage diabetes, with little consideration of stress and financial levels.” We wanted to measure how people with diabetes feel about the care they get from their healthcare providers.
This is the second of three articles that will explore the many amazing things that we learned from the Healthcare Satisfaction Survey. These three deep dives are organized around the most jaw-dropping results:
- 47.1 percent of people with diabetes rarely or never discuss mental health at healthcare appointments.
- Black and Latino people with diabetes are about half as likely to feel supported or empowered at healthcare appointments as white patients.
- 22.7 percent of people with diabetes rarely or never discuss diet or exercise with their healthcare providers, and about 50 percent rarely or never discuss their lab results.
What We Know About Healthcare Inequality
The American healthcare system has an inequality problem, to put it mildly. White Americans are much healthier than people that identify as Black, Hispanic, or American Indian and Alaska Native; whites report better healthcare experiences and outcomes almost across the board. Why? For one thing, the American medical establishment is riddled with bias. For another, our lack of a strong social healthcare system means that economically disadvantaged patients are frequently stuck with lower-quality treatment. A Commonwealth Fund report found that the United States had by far the largest income-based healthcare disparities of any comparable nation. The result is that the patients groups that need the most help are, conversely, the least likely to receive the most effective therapies.
The most explosive consequence of the treatment gap is the widespread rationing of insulin, but the disparities also show up in more subtle and pernicious ways, as our survey helps to illuminate.
The Thrivable Panel
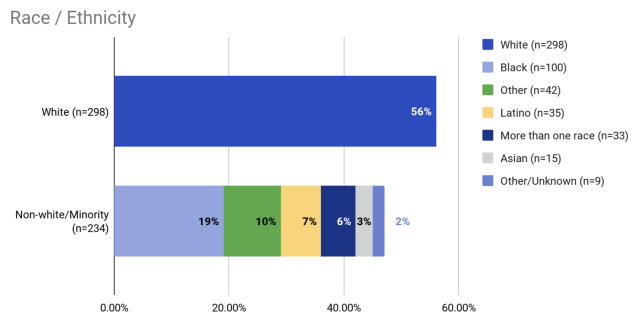
Our 532 survey panelists were selected by Thrivable to create a nationally representative sample. The participants hailed from all parts of the United States, were of all different ages, and had all different kinds of insurance. Fifty-six percent of respondents identified as white alone, very close to the proportion found in the latest U.S. census; the remainder identified as belonging to one or more racial or ethnic minorities.

Our analysis will concentrate on three groups: white, Black, and Latino.
The panel was also socioeconomically diverse, featuring many participants both below the poverty line and above six figures, and at every income level in between.

The Results: Race/Ethnicity and Access to Diabetes Expertise
Perhaps the most fundamental manifestation of America’s racial and ethnic healthcare problem is unequal access to healthcare resources — an issue that was only amplified by the COVID-19 pandemic.
White respondents were more than twice as likely (55 percent) to see an endocrinologist as Black (22 percent) and Latino (17 percent) respondents. When we broke down the data by diagnosis — to ensure that differing rates of type 1 and 2 diabetes didn’t account for the gap — we found the same association. 34 percent of White Americans with type 2 diabetes, for example, see an endocrinologist, compared with only 16 percent of Blacks and 14 percent of Latinos.
It’s an eye-opening finding. White Americans, clearly, are far more likely to be treated by a specialist. Other results told a similar story:
- Black and Latino respondents were significantly less likely to rate their provider as “extremely knowledgeable.”
- Black and Latino respondents were almost half as likely to discuss new technology at their healthcare visits.
- Black and Latino respondents were much less likely to discuss new treatments at their healthcare visits.
This commentary shouldn’t be construed to imply that family doctors, nurse practitioners, and diabetes educators are unable to give patients the support and care they need. Many people with diabetes are quite pleased with the medical care they receive from practitioners other than endocrinologists. Our data does show, however, that those who see an endocrinologist are more likely to report feeling somewhat or very supported, empowered, and validated than those who see a general practitioner or nurse practitioner.
That’s probably especially true for those living with advanced diabetic complications, which are experienced disproportionately by Black and Hispanic people. It could be that the patients that are most in need of advanced care are those that are paradoxically least likely to receive it. Recognizing this problem, as well as many others, the Endocrine Society recently pledged to eradicate racism within its ranks.
This isn’t an easy problem to solve. There is a nationwide endocrinologist shortage. With too few endos to go around, it’s likely already disadvantaged communities that get the short end of the stick.
Although our panelists all had diabetes already, the same access issues can also make the development of diabetes more likely in the first place. Several minority groups have much higher rates of type 2 diabetes than do white Americans, a difference that is suspected to result from social determinants of health, including healthcare access, as much as or more so than genetic factors.
One of our simplest survey questions turned out to be one of the most illuminating. We asked our participants how easy it was to book healthcare appointments. We learned that white patients have a much easier time booking appointments, with 73 percent reporting that it was “very easy” to schedule appointments. Only 53 percent of Black respondents and 43 percent of Latinos gave the same answer. Could there be a more concise illustration of healthcare access disparities?
Race/Ethnicity and Emotional Support
As we hinted in our first analysis of our survey data, Black and Latino respondents appear to be far less satisfied and comforted by the medical care they are receiving.
The problems start before the appointment even begins, as Black and Latino participants reported much higher levels of anxiety before seeing their healthcare providers.

The converse is also true. White survey participants were about three times as likely to report feeling “very calm” before and during appointments.
An uncomfortable medical appointment might be more impactful than it initially appears. Anxiety can be a big part of life with diabetes, in multiple ways. Anxiety may be both a cause of diabetes progression and a symptom of the difficulty entailed by diabetes management. It’s a vicious cycle, one that ideally would never be touched off by a visit to the professional charged with ensuring one’s well-being.
Things don’t get much better during and after the appointment:
- White respondents were significantly more likely to say they feel very supported than Black and Latino respondents (44 percent vs. 20 percent and 17 percent, respectively).
- White respondents were significantly more likely to say they feel very empowered than Black and Latino respondents (57 percent vs. 29 percent and 31 percent, respectively).
- White respondents were significantly more likely to say they feel very validated than Black and Latino respondents (37 percent vs. 24 percent and 23 percent, respectively).
Inequality — or, at the very least, the perception of inequality — impacts members of the diabetes community immediately, before, during, and after healthcare appointments. It’s not easy to manage your condition optimally if you feel that you aren’t receiving optimal support.
Income and Provider Access
Race and ethnicity aren’t everything — America’s healthcare inequality problem also shows up in a big way when we compare the haves and have-nots.
Our survey provides a clear picture: As patients become wealthier, they are increasingly able to access an entire team of experts to optimize their diabetes care. Less affluent patients are more likely, on the other hand, to make do with a single professional.
- Nearly 50 percent of respondents that reported an income under $15,000 see a general practitioner for their diabetes. In a remarkable contrast, only a single survey participant of the 48 that reported an income over $150,000 sees a GP. That’s a mere 2 percent.
- Certified diabetes educators (CDCESs) and diabetes coaches, although they have fewer credentials than medical doctors and nurse practitioners, appear to be luxury items. We’re big fans of CDCESs and diabetes coaches, who can often drill down into the daily reality of diabetes management with even greater detail than endocrinologists can. But almost nobody earning less than $50,000 saw one of these professionals.
- Registered dieticians were likewise all but unavailable to those with the lowest incomes.
Income and Therapies
It’s tough to thrive with diabetes if you don’t have access to medical technologies and therapies. And access in America, compared with some other parts of the world, is profoundly unequal.
About 26 million Americans have no health insurance at all, slightly under 10 percent of the population. Even for those that do have insurance, however, advanced therapies like an insulin pump, a continuous glucose monitoring (CGM) system, or the most-effective drugs can remain out of reach. For the millions of Americans on high-deductible plans, for example, insurance might offer almost no reimbursement for a CGM system at all.
Our survey found the same pattern. For example, there was a positive correlation between income and CGM usage. Only 28.9 percent of those earning less than $15,000 used a CGM, compared with 100 percent of those in the highest income bracket.
In order to extricate the effect of race or ethnicity, we also looked at the numbers for white Americans alone. They told much the same story. White respondents earning less money were less likely to discuss new technology and new treatments with their healthcare providers.
Even in nations with more robust socialized healthcare systems, such as Canada, there is a correlation between lower income and a higher rate of severe diabetes outcomes. In America, these associations are just getting worse as wealth disparity gaps keep growing.
Doctors and endocrinologists cannot reverse America’s wealth distribution problems by themselves. But they can pledge to recommend the best treatments to their patients without prejudice and advocate on their behalf to insurers. As our Healthcare Satisfaction Survey shows, there’s a lot of work to be done to overcome America’s systemic healthcare equity problems.












Wittiest stocks:: Avalo Therapeutics Inc (NASDAQ:AVTX 0.00%), Nokia Corp ADR (NYSE:NOK 0.90%)
There are two main reasons why moving averages are useful in forex trading: moving averages help traders define trend recognize changes in trend. Now well…

Spellbinding stocks: LumiraDx Limited (NASDAQ:LMDX 4.62%), Transocean Ltd (NYSE:RIG -2.67%)
There are two main reasons why moving averages are useful in forex trading: moving averages help traders define trend recognize changes in trend. Now well…

Seducing stocks: Canoo Inc (NASDAQ:GOEV 5.43%), Ginkgo Bioworks Holdings Inc (NYSE:DNA -1.12%)
There are two main reasons why moving averages are useful in forex trading: moving averages help traders define trend recognize changes in trend. Now well…